If you’ve recently undergone a sleep evaluation and received results you’re not quite sure how to interpret, you’re not alone. One of the most commonly misunderstood values in sleep medicine is the respiratory disturbance index, and understanding what it means could be an important step in addressing your sleep health.
When your doctor orders a sleep study, the report usually contains several metrics that measure how your breathing behaves during the night. Among these, the RDI in sleep study results is a particularly comprehensive indicator. Unlike some other measurements, it captures a broader picture of how disrupted your breathing actually is.
This guide will walk you through what the respiratory disturbance index is, how it’s measured, what counts as normal, and how it compares to similar metrics like the apnea-hypopnea index (AHI). By the end, you’ll have a much clearer understanding of your results and what your next steps might look like.
What Is the RDI Index and How Is It Measured?
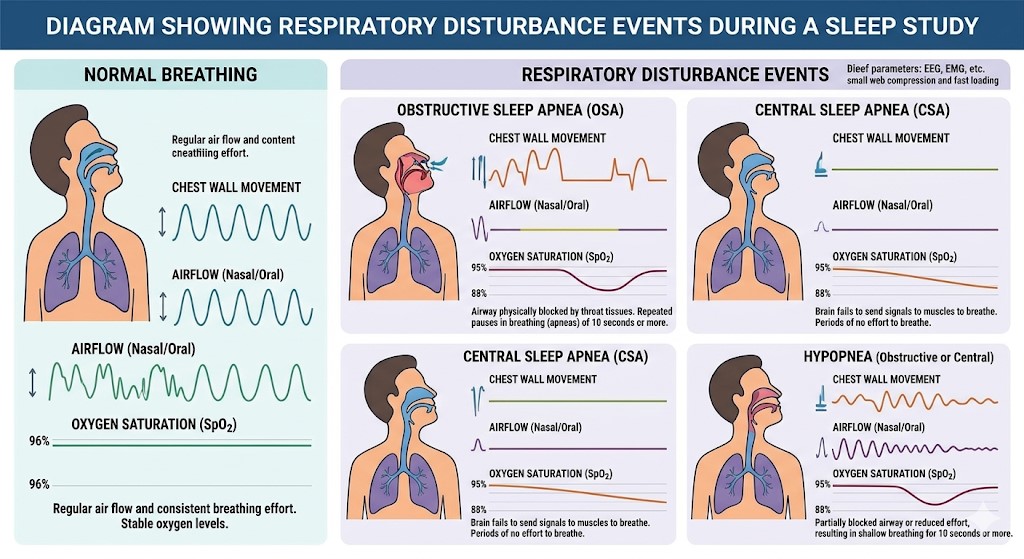
The respiratory disturbance index — commonly referred to as the RDI index — is a metric used in sleep medicine to quantify the average number of respiratory disturbances a person experiences per hour of sleep. These disturbances include:
- Apneas — complete pauses in breathing lasting at least 10 seconds
- Hypopneas — partial reductions in airflow that disrupt sleep quality
- Respiratory effort-related arousals (RERAs) — subtle breathing irregularities that cause brief awakenings without meeting the technical criteria for apnea or hypopnea
That last category — RERAs — is what makes the RDI index particularly useful. Many patients experience significant nighttime sleep fragmentation caused primarily by RERAs, which would go undetected if only looking at apneas and hypopneas alone.
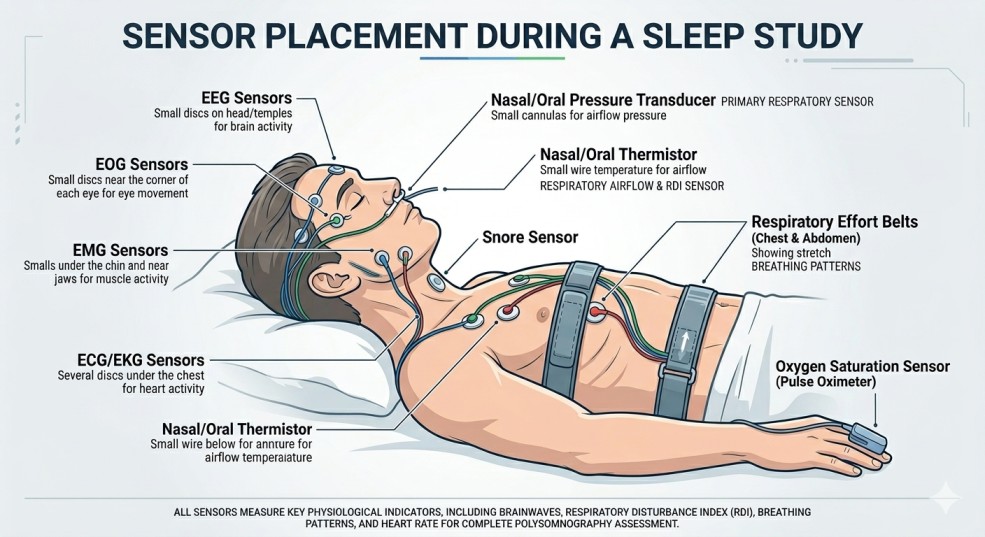
Your respiratory rate while sleeping is closely monitored during a sleep study using sensors that track airflow, oxygen saturation, chest movement, and brain activity. Technicians and sleep physicians use this data to calculate your RDI score. You can learn more about how your respiratory rate while sleeping affects overall sleep health on our blog.
Understanding What Is Normal RDI in Sleep Study Results
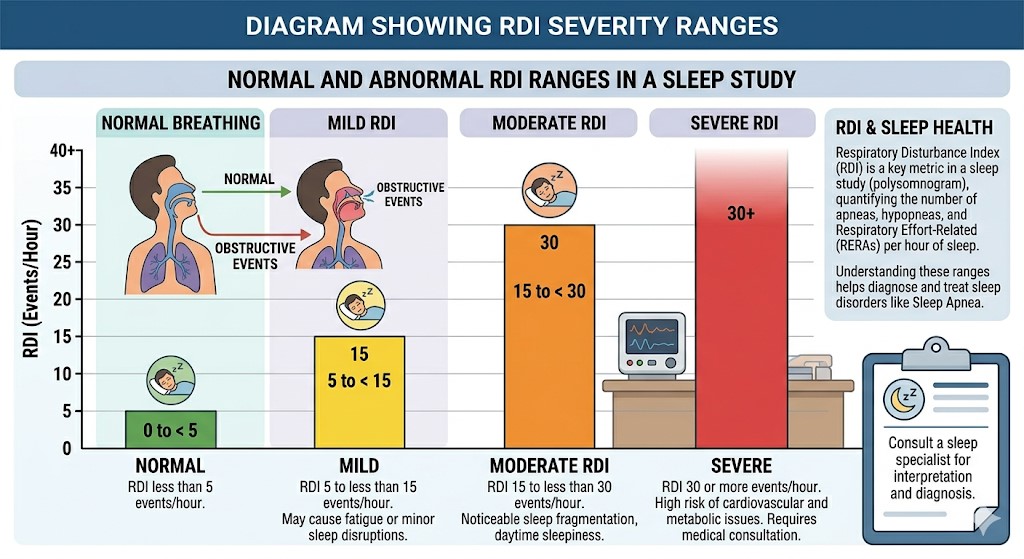
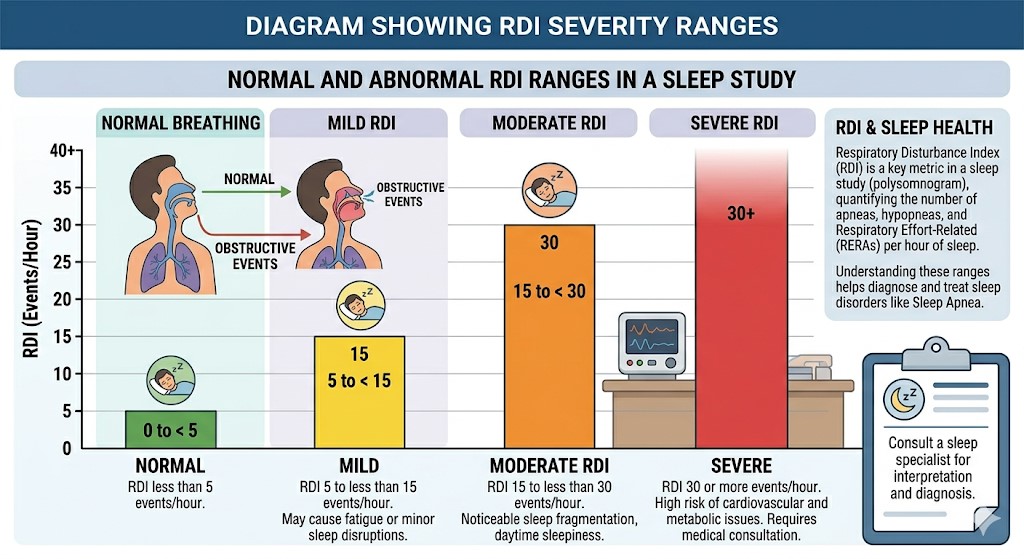
A common question patients ask is: what is normal RDI in sleep study reports? Generally, clinicians use the following reference ranges:
- Normal: RDI below 5 events per hour
- Mild sleep-disordered breathing: RDI of 5–14
- Moderate sleep-disordered breathing: RDI of 15–29
- Severe sleep-disordered breathing: RDI of 30 or higher
It’s worth noting that some guidelines may use slightly different cut-offs depending on the clinical setting or the type of sleep study used (in-lab polysomnography vs. home testing). For example, clinical thresholds and diagnostic criteria are commonly guided by organizations such as the American Academy of Sleep Medicine (AASM), which provide standardized recommendations used by sleep specialists. Your physician will interpret your results in context with your symptoms, medical history, and other health factors.
If your RDI is elevated, it doesn’t automatically mean you have a severe condition — but it is a signal worth discussing with your doctor. Even mild disturbances, when occurring frequently throughout the night, can leave you feeling unrested, affect your mood, and contribute to longer-term health concerns.
Another metric worth understanding in this context is the oxygen desaturation index, which tracks how often your blood oxygen levels drop during sleep — often a companion metric to the RDI.
AHI vs RDI: What’s the Difference?
One of the most frequent points of confusion in sleep medicine is the distinction between AHI vs RDI. Both are used to measure breathing disruptions during sleep, but they’re not the same thing.
The Apnea-Hypopnea Index (AHI) counts only apneas and hypopneas per hour. The RDI goes further by also including respiratory effort-related arousals (RERAs). This means the RDI is always equal to or higher than the AHI for any given patient.
Here’s why that distinction matters: some people have an AHI that falls within normal limits but still struggle with poor sleep quality, daytime fatigue, and morning headaches. In these cases, their RERAs — captured by the RDI — may be the culprit. Without measuring the RDI, those breathing-related disruptions might go completely unrecognized.
For a broader, patient-friendly overview of sleep apnea and how these metrics are used in diagnosis, you can also refer to resources from the National Heart, Lung, and Blood Institute (NHLBI).
In clinical practice, the choice of which metric to use often depends on the type of sleep study performed and the physician’s clinical judgment. Home sleep apnea tests, for instance, may not always capture RERAs as reliably as in-lab polysomnography.
Regardless of which number is elevated, both metrics point toward potential RDI sleep apnea-related concerns that are worth evaluating further.
What to Do If Your RDI in Sleep Study Results Are Elevated
Finding out that your RDI in sleep study results are higher than normal can feel overwhelming, but knowledge is the first step toward better sleep. Here are some practical paths forward:
Speak With a Sleep Specialist
A board-certified sleep physician can interpret your results in full context and recommend appropriate next steps, which may include lifestyle changes, positional therapy, oral appliances, or PAP therapy.
Consider Targeted Exercises
Research suggests that certain myofunctional exercises may help reduce the frequency of respiratory disturbances. Explore our guide on exercises for sleep apnea to learn about options you can try at home alongside professional treatment.
Start With a Home Sleep Test
If you haven’t yet had a formal sleep evaluation, or if you’d like a convenient first step, an at-home sleep test can provide valuable baseline data about your nighttime breathing. It’s a simple, non-invasive way to get started without an overnight visit to a sleep lab.
Conclusion: Take Your Sleep Health Seriously
Your sleep study results contain valuable information — and the respiratory disturbance index is one of the most telling indicators of how well your airway is functioning while you sleep. Whether your score is mildly or significantly elevated, understanding what it means puts you in a better position to take action.
From consulting a sleep specialist to exploring lifestyle interventions, there are many effective options for addressing elevated RDI in sleep study findings. Don’t wait to take the first step.
Ready to find out where you stand? An at-home sleep test is a simple, convenient way to begin your journey toward more restful, restorative nights. Order yours today and get the answers you deserve.
Frequently Asked Questions
What does a high RDI mean?
A high RDI indicates that you’re experiencing a significant number of breathing-related disruptions per hour of sleep. Depending on the severity, this may point to sleep-disordered breathing that warrants clinical evaluation and possibly treatment.
Can you have a normal AHI but a high RDI?
Yes. Because the RDI includes respiratory effort-related arousals (RERAs) that the AHI does not, it’s possible for your AHI to appear normal while your RDI is elevated. This is one reason why a comprehensive sleep evaluation is so important.
Is RDI the same as sleep apnea?
Not exactly. A high RDI indicates sleep-disordered breathing, which encompasses a spectrum of conditions including snoring, upper airway resistance syndrome, and obstructive sleep apnea. Your physician will use the RDI along with your symptoms and other test results to determine a diagnosis.
How is RDI calculated during a sleep study?
The RDI is calculated by dividing the total number of respiratory events (apneas + hypopneas + RERAs) by the total hours of sleep recorded during the study. The resulting number represents disturbances per hour.
What’s a good RDI score?
An RDI below 5 events per hour is generally considered within the normal range. An RDI between 5 and 14 suggests mild sleep-disordered breathing, while scores of 15 or higher indicate moderate to severe disruption.




{kind=link}